This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In this episode, I’ll discuss an article about timing of amiodarone for out-of-hospital, shock-refractory cardiac arrest. In the early group, patients who received amiodarone has statistically signficantly higher rates of survival to hospital admission, survival to discharge, and functional survival when compared to placebo.
Patients were matched based on hospital, diagnosis, and 28 clinical factors. The authors concluded: On average, among a large sample of adult inpatients who ultimately received broad-spectrum antibiotic therapy, delaying initiation of a broad-spectrum antibiotic was not associated with worse outcomes. Mortality was 8.7%
In this episode, I’ll discuss the impact of giving epinephrine before defibrillation to in-hospital cardiac arrest (IHCA) patients with shockable rhythms. The main outcome examined epinephrine administration before first defibrillation and its association with hospital-level rates of risk-adjusted survival.
Unfortunately the ability to do so without using a send-out laboratory is not widespread among hospitals. To get access to my free download area with 20 different resources to help hospital pharmacists go to pharmacyjoe.com/free.
Treatment also was responsible for a lower length of hospital stay when compared to control. To get access to my free download area with 20 different resources to help hospital pharmacists go to pharmacyjoe.com/free. The relative risk in favor of treatment was 0.56.
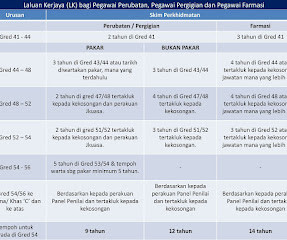
What can I expect once I entered hospital provisional registered pharmacist training? In most hospitals, you first introduction to your workplace is through an induction period during which you are shown many different areas and meet many new people. What is the career pathway of a government hospital pharmacist?
In this episode, I’ll discuss torsemide vs furosemide for symptoms and quality of life among patients hospitalized for heart failure. Episode 824: Torsemide vs Furosemide – Which Is Better For Symptoms and Quality of Life Among Patients Hospitalized for Heart Failure? appeared first on Pharmacy Joe.
In this episode, I’ll discuss the lowest effective dose of IV or IM haloperidol for elderly hospitalized patients with agitation. Secondary outcomes were the hospital length of stay, utilization of restraints, and discharge outcomes (to a facility when admitted from home) between dosage groups.
In this episode, I’ll discuss an article about timing of amiodarone for out-of-hospital, shock-refractory cardiac arrest. In the early group, patients who received amiodarone has statistically signficantly higher rates of survival to hospital admission, survival to discharge, and functional survival when compared to placebo.
In this episode, I’ll discuss what an inpatient pharmacist needs to know about the outpatient CDC opioid guidelines. This means that you can’t simply use one style of opioid dosing while the patient is in the hospital and instantly change to something else when the patient goes home.
To get access to my free download area with 20 different resources to help hospital pharmacists in their practice go to pharmacyjoe.com/free. If you like this post, check outmy book A Pharmacists Guide to Inpatient Medical Emergencies: How to respond to code blue, rapid response calls, and other medical emergencies. <–
Episode 840: A Rare Disease Resource Every Hospital Pharmacist Should Know About Subscribe on iTunes , Android , or Stitcher There exists a large number of rare diseases that any given hospital pharmacist might encounter once in their practice, if at all.
Episode 840: A Rare Disease Resource Every Hospital Pharmacist Should Know About Subscribe on iTunes , Android , or Stitcher There exists a large number of rare diseases that any given hospital pharmacist might encounter once in their practice, if at all.
The database used in the analysis draws from over 600 US hospitals. The primary outcome focused on the volume of resuscitative IV fluid administered before the end of hospital day 1 and mortality. To access my free download area with 20 different resources to help you in your practice, go to pharmacyjoe.com/free.
Episode 891: The Half-Dose Alteplase Study You’ve Always Wanted Subscribe on iTunes , Android , or Stitcher Members of the Hospital Pharmacy Academy have access to trainings on how to run a journal club, and biostatistics for journal club in addition to hundreds of other trainings to help you in your practice.
To get access to my free download area with 20 different resources to help hospital pharmacists go to pharmacyjoe.com/free. If you like this post, check outmy book A Pharmacists Guide to Inpatient Medical Emergencies: How to respond to code blue, rapid response calls, and other medical emergencies. <–
In this episode, I’ll discuss new orders for fentanyl patches in the hospital setting. Episode 661: Fentanyl Patch Safety in Hospitals Subscribe on iTunes , Android , or Stitcher Transdermal fentanyl patches are contraindicated in the treatment of acute pain or in patients who are not opioid tolerant.
In this episode, I’ll discuss colchicine in patients admitted to hospital with COVID-19. Episode 660: Does colchicine work in patients admitted to hospital with COVID-19? mg orally 12 hours later and twice daily thereafter for 10 days or until hospital discharge. appeared first on Pharmacy Joe.
In this episode, I’ll discuss what I feel is the most important thing in hospital pharmacy practice. Episode 710: The Most Important Thing in Hospital Pharmacy Practice Subscribe on iTunes , Android , or Stitcher Twenty years ago I transitioned from community to hospital practice.
Expanding the Acute Stroke Thrombolysis Window to 24 Hours “ The editorialist cautions that the results of this trial need to be replicated in other populations, and for real-world implementation of the protocol used in this study, hospitals would need perfusion-imaging capability. hours from time last know well?
In this episode, I’ll discuss the continuation of newly prescribed gabapentin for acute pain management after hospital discharge. A group of authors recently published a retrospective cohort study characterizing the use of newly prescribed gabapentin in hospitalinpatients. Episode 961: Is that gabapentin just temporary?
Episode 832: Savings realized by the redistribution of short-dated emergency medications Subscribe on iTunes , Android , or Stitcher Placing emergency medications throughout the hospital in drug boxes is essential to ensure their availability when emergencies arise. However, this leads to a large number of medications that expire unused.
In this episode, I’ll discuss whether 3 days of beta-lactam use is enough to treat CAP in non-ICU hospitalized patients. Episode 620: Is 3 days of beta-lactam use enough to treat CAP in non-ICU hospitalized patients? To access my free download area with 20 different resources to help you in your practice, go to pharmacyjoe.com/free.
Episode 599: Enoxaparin is associated with lower rates of mortality than unfractionated Heparin in hospitalized COVID-19 patients Subscribe on iTunes , Android , or Stitcher Managing coagulopathies in patients hospitalized with COVID-19 is one of the more challenging aspects of care for these patients.
The authors analyzed data from over 24,000 adult patients with severe traumatic brain injury who received a vasopressor within the first 2 days of hospital admission. In-hospital mortality was the primary outcome while secondary outcomes examined included hospital length of stay (LOS) and ICU LOS.
In this episode, I’ll discuss amiodarone vs lidocaine for in-hospital cardiac arrest. Subscribe on iTunes , Android , or Stitcher The ACLS guidelines suggest either amiodarone or lidocaine for in-hospital cardiac arrest that is due to ventricular tachycardia or ventricular fibrillation (VT/VF).
In this episode, I’ll discuss the impact of giving epinephrine before defibrillation to in-hospital cardiac arrest (IHCA) patients with shockable rhythms. The main outcome examined epinephrine administration before first defibrillation and its association with hospital-level rates of risk-adjusted survival.
To a pharmacist, it makes sense that pharmacy-driven medication histories for patients admitted to the hospital would provide benefits to patients in the same way that having a cardiologist manage heart failure over a generalist would to a heart failure patient. This difference was statistically significant.
Episode 832: Savings realized by the redistribution of short-dated emergency medications Subscribe on iTunes , Android , or Stitcher Placing emergency medications throughout the hospital in drug boxes is essential to ensure their availability when emergencies arise. However, this leads to a large number of medications that expire unused.
In this episode, I’ll discuss the effect of unnecessary long-term continuation of newly initiated stress ulcer prophylaxis in the ICU on morbidity and mortality after hospital discharge. However, PPI use often continues after ICU and hospital discharge without indication. All of these differences reached statistical significance.
Secondary outcomes were the rate of clinical recovery, the incidence of drug-related adverse events, ICU and hospital mortality. Additionally, there were no differences between groups in rates of nephrotoxicity, clinical recovery, ICU and hospital survival.
There were no significant differences found in any of the secondary outcomes including conversion to sinus rhythm, bradycardia, vasopressor duration, intensive care unit (ICU) and hospital length of stay, and hospital mortality.
The authors concluded: This study did not support the longstanding rule of thumb for K+ supplementation and found a smaller rise in K+ for every 10 mEq of K+ delivered when looking at patients holistically over a full hospitalized day. Loop diuretics were the drug class identified to have the greatest impact on this metric.
The authors concluded: This study did not support the longstanding rule of thumb for K+ supplementation and found a smaller rise in K+ for every 10 mEq of K+ delivered when looking at patients holistically over a full hospitalized day. Loop diuretics were the drug class identified to have the greatest impact on this metric.
The primary outcome the authors examined was the rate of in-hospital mortality or transfer to hospice care. The rate of in-hospital mortality or hospice was 4.6% The rate of in-hospital mortality or hospice was 4.6% In the overall cohort, 40% of the patients were reversed and 60% were not reversed.
The primary outcome the authors examined was the rate of in-hospital mortality or transfer to hospice care. The rate of in-hospital mortality or hospice was 4.6% The rate of in-hospital mortality or hospice was 4.6% In the overall cohort, 40% of the patients were reversed and 60% were not reversed.
In this episode, I’ll discuss the continuation of newly prescribed gabapentin for acute pain management after hospital discharge. A group of authors recently published a retrospective cohort study characterizing the use of newly prescribed gabapentin in hospitalinpatients. Episode 718: Is that gabapentin just temporary?
In this population, the receipt of linezolid was not associated with a statistically significant different absolute risk reduction of in-hospital mortality compared with clindamycin. To access my free download area with 20 different resources to help you in your practice, go to pharmacyjoe.com/free.
Shout out to “Pharmacy Hend” who is a podcast listener, Hospital Pharmacy Academy member, and one of the authors on this article. To get access to my free download area with 20 different resources to help hospital pharmacists in their practice go to pharmacyjoe.com/free. The huddle process worked like this: 1.
The primary exposure examined was the vasopressor choice (phenylephrine versus norepinephrine) within the first 2 days of hospital admission and the primary outcome was in-hospital mortality. To get access to my free download area with 20 different resources to help hospital pharmacists go to pharmacyjoe.com/free.
The primary exposure examined was the vasopressor choice (phenylephrine versus norepinephrine) within the first 2 days of hospital admission and the primary outcome was in-hospital mortality. To get access to my free download area with 20 different resources to help hospital pharmacists go to pharmacyjoe.com/free.
Such an example was recently published in JAMA of the Epic Sepsis Model (ESM), a proprietary sepsis prediction model that was widely used at hundreds of US hospitals to predict the development of sepsis in inpatients. To access my free download area with 20 different resources to help you in your practice, go to pharmacyjoe.com/free.
Mean hospital length of stay was 2 days shorter for the tranexamic acid group (5.7 ± 2.5 To access my free download area with 20 different resources to help you in your practice, go to pharmacyjoe.com/free. Patients in the active group got undiluted inhalations of IV form of tranexamic acid 500 mg/5 ml 3-4 times a day.
Mean hospital length of stay was 2 days shorter for the tranexamic acid group (5.7 ± 2.5 To access my free download area with 20 different resources to help you in your practice, go to pharmacyjoe.com/free. Patients in the active group got undiluted inhalations of IV form of tranexamic acid 500 mg/5 ml 3-4 times a day.
We organize all of the trending information in your field so you don't have to. Join 11,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content